SECTIONS: 4 | 6 | 7 | 8 | 9 | 10 | 12 | 13 | 19 | 24

-
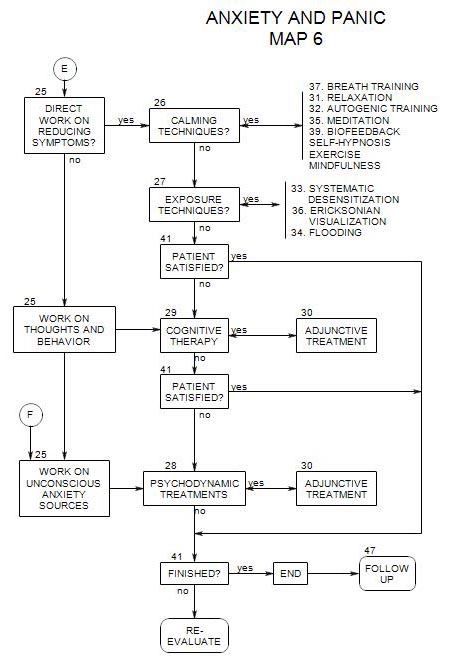
Follows Section 27 on Map 6
33a. History and Theory
Originally, Wolpe [1958] demonstrated that fear reactions in cats could be reduced by having them eat in the presence of an attenuated version of the feared object. He then had them eat in the presence of fear stimuli with increasing saliency, in each case continuing until the fear was reduced. Wolpe argued that the eating inhibited the fear reaction.
With human subjects, relaxation was substituted for eating as a response inconsistent with fear. However, other substitutions might also be made. The patient’s control over the situation could also be varied, to inhibit the fear reaction.
In addition, exposure and habituation to the fear-arousing stimulus may be sufficient, without relaxation, in cases of low arousal. However, with high arousal exposure may increase the fear reaction. [Wachtel, 168-169]
An additional factor, the therapist’s approval for the patient’s success in overcoming fear reactions, may be helpful. [Wachtel, 174]
33b. Technique
Systematic desensitization involves several steps: [Wolpe, 1969]
- Find out what stimuli lead a person to be anxious.
- List the stimuli in a hierarchy, from least to most frightening.
- Train the person in deep muscle relaxation [ Section 31 ].
- Start by presenting a stimulus at the least threatening end of the hierarchy, while the person is in a relaxed state He/she focuses on the stimulus for a period of time, until any anxiety dissipates.
- Present another stimulus slightly higher on the hierarchy.
- Continue, extinguishing anxiety for successively more threatening stimuli until the person can tolerate the most threatening without anxiety.
33c. Imaginal Desensitization
This is the form that systematic desensitization most often takes.
An attempt is made to reduce the person’s anxiety level by presentation of imagined encounters with the feared object or situation.
For example, a person with a fear of cats might set up a hierarchy of imagined situations, going from
- Having a cat in a cage, in another room in the building, and the door is closed.
- The door is open.
- The cage is brought into the same room but is at the far side of the room.
- The cat is on a leash on the other side of the room.
The list continues, with steps decided on together, until the patient is imagining holding the cat and petting it.
In this approach, having made the list, the patient relaxes and then is asked to think of the top situation on the list, and continue to think of it while once again relaxing. Then the patient is asked to think of the next situation and helped to relax once more. Eventually – and this may take several sessions, the patient ought to be able to relax while thinking the most frightening thought.
33d. Modified Imaginal Desensitization
There are problems with the pure imaginal approach. For one thing, some patients don’t imagine well or vividly. The minds of others may wander. It is, after all, difficult to stay focused on any stimulus, and harder if it’s something frightening.
One solution is to add props: drawings, photographs, audio tapes of the feared situation or creature, and so on.
For example, a sequence of large and small photographs of cats can be presented across the room. Some of the photos can be more frightening than others – possibly starting with kittens asleep or at play. Then the same photos can be moved closer and closer, until the person is holding them and examining them.
33e. Virtual Reality Presentation
This is another step in the direction of increased realism. Here the presentations are computer generated and the increasing frightfulness closely regulated. In some versions, the patient dons special equipment that gives an even closer approximation to reality.
33f. In Vivo Desensitization
Here the person is confronted with the actual situation or object feared, rather than an imagined or simulated version of it.
As described by Ross, there are several key elements
- The patient makes his/her own set of long term behavioral goals.
- The long term goals are then broken down into small incremental steps.
- The patient keeps a daily record of activities done in completing the steps. This record includes sufficient detail so that review after a period of time will clearly show the person’s level of approach to the long-term goal and reactions to that level.
The therapist’s job includes-
- providing help in formulating the steps and adjusting them according to the person’s reactions.
- encouraging the patient to continue, in part by reminding him/her of progress made.
- helping with anticipatory anxiety.
- giving hints to deal with fear of loss of control.
33g. Variations:
- Combinations of the two approaches, possibly doing imaginal desensitization in the office and in vivo as homework.
- Combinations can be carried out in the office also, typically starting with imaginal and moving to in vivo. For example, if the person fears cats, you could start with fantasized images of cats, go on to photos across the room, then move the photos closer, then a real cat across the room and then slowly move the cat closer.
References:
Ross, 1996″
Wolpe, J.1969
Wachtel, Paul, 1977
Zane, 1996