SECTIONS: 4 | 6 | 7 | 8 | 9 | 10 | 12 | 13 | 19 | 24

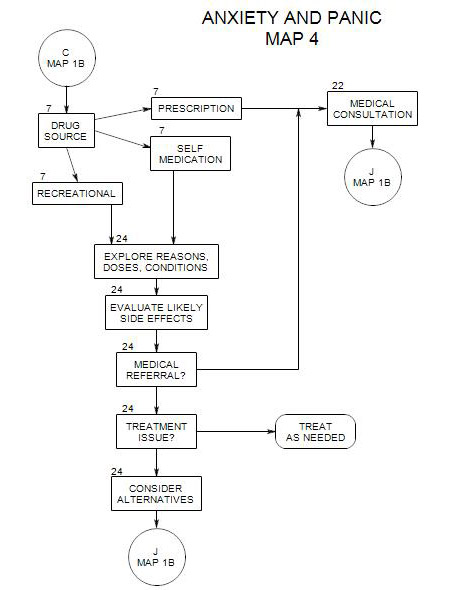
- Follows from Section 6 [Medical Disorders] on and Map 3
Also follows from Section 7 [Drug Reactions] and Section 24 on Map 4
We may refer to a physician early on in treatment if we suspect that a person’s anxiety is caused in part either by a medical disorder or a drug reaction. See Section 30 for medical treatment
22a. Obtaining the Person’s Permission
The patient needs to know the reason for the medical consultation. It can be very explicit, if you suspect a specific medical disorder as the source of the person’s anxiety, or more open, if you are less sure.
The person needs to give written permission for you to contact his/her physician, if you are to be involved in that process. Or he/she may simply make his/her own appointment. If he/she refuses you permission to make the call, it may be valuable to understand the reason[s] for the refusal. If he/she refuses to go for a consultation, those reasons can be important to know.
22b. Gathering the Information
This should be done, if possible, before making the referral. See Section 6 for a discussion of possible medical disorders and Section 7 and Section 24 for possible drug reactions.
22c. Making the Referral
Keep lists of the person’s symptoms, drugs and medical conditions and pass them along with the referral.
A typical referral could be for a physical examination, along with laboratory tests for anemia, electrolyte balance, calcium regulation, thyroid function and cardiac function. (Lesser, 1996, p. 37)
Reasons for contacting the physician first
Reasons include-
- letting him/her know that your patient is coming
- discussing the person’s needs and symptoms, especially if there are some that the person might not mention.
- explaining your concerns about any of the drugs [prescription or otherwise] that the person is taking.
- establishing or maintaining a working relationship with the physician. (Beitman and Saveanu, 2005, p. 431)
Reasons not to contact the physician first
- Your patient is going to a clinic and doesn’t know who will be treating him/her
- It might appear to your patient to be infantilizing
22d. Follow-up on a Medical Consultation
It is valuable to most patients to have a discussion about the results of the examination, regardless of the outcome. If you consider all the implications of the medical results with your patient, it will help to define the scope of treatment and to establish a collaborative relationship.
This might especially be true if the person is self-medicating out of suspicion of physicians, or the ineffectiveness of prior treatments.
22e. Medical Management
It may be for some medications that the physician will want to see your patient regularly, to manage dosage and monitor its effect. This could affect your treatment of the person, so it would be useful to know the physician’s concerns and their implications for the person’s psychological symptoms.
22f. Possible Termination
It is possible that the person’s entire problem is disability or drug related, that he/she has no additional psychological baggage, and that termination is the appropriate next step. It is unlikely, but possible. Having a relationship with the patient’s physician will be helpful in making that decision.
22g. Follow-up on other drug use
You also may need to bring the use of recreational drugs into the treatment, if they are dangerous or if they are illegal and the person is at risk from using them.