SECTIONS: 4 | 6 | 7 | 8 | 9 | 10 | 12 | 13 | 19 | 24

-
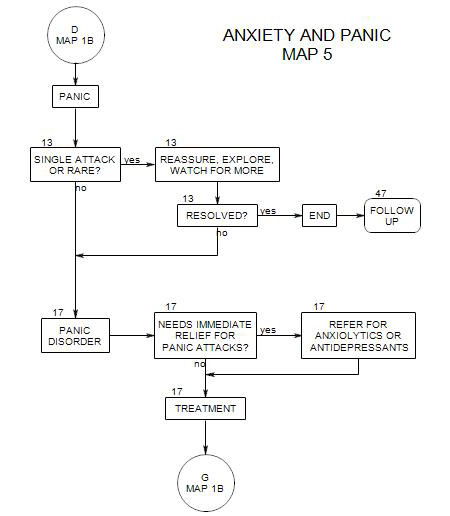
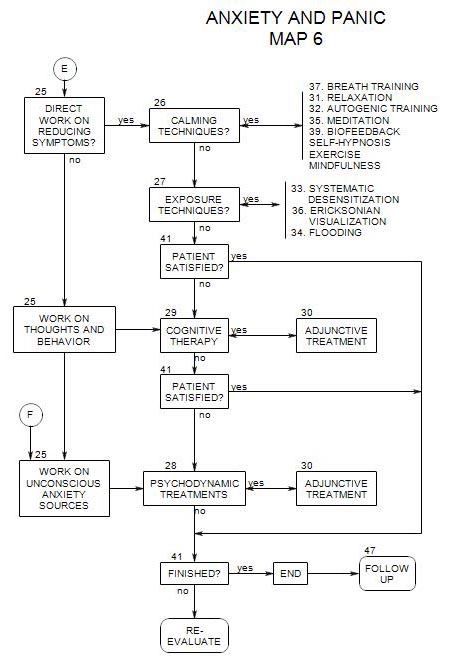
Follows Section 25 on Map 629a. General Principles
In cognitive therapy, anxiety is seen as a consequence of the person’s perceptions, expectations and interpretations of events, rather than as consequences of the events themselves. Treatment involves identifying the thoughts or cognitions that relate to the fear reaction and challenging or refuting them (Hofmann and DiBartolo, 1997, pp. 59-64).
An anxious person scans internally and externally for dangers. The hypervigilance leads to inaccurate estimates of danger and/or misattribution of the source of the symptom.
The three components of anxiety [cognitions, behavior, emotions] affect each other. Cognitive therapy attempts to interrupt the complex interplay among them by a focus on the person’s negative cognitions – and by replacing those negative cognitions by more positive ones.
Characteristics of anxious cognitions:
- They are future-oriented predictions of danger or threat.
- The danger could be physical [such as a heart attack] or psychological [like embarrassment].
- The predicted symptoms are seen as uncontrollable.
- They occur automatically in response to often subtle cues.
Most often encountered cognitive distortions include-
- all-or none thinking.
- jumping to conclusions.
- exaggerating or minimizing.
- disqualifying the positive.
- should statements.
- Labeling.
The goal of treatment is cognitive modification. Behavioral exercises are also directed toward this goal.
29b. Technique
Following are common steps in the cognitive treatment of a disorder (Hofmann and DiBartolo, 1997, pp. 63-78):
- Focus on the main therapeutic problem: one or two core negative irrational beliefs that the patient has about him/herself.
- The patient identifies issues he/she wants to target during treatment.
- Identify the patient’s anxious cognitions.
- Treat irrational thoughts as hypotheses to be tested, and the patient as an experimenter or scientist, whose job is to evaluate the hypotheses.
- Challenge aspects of the person’s thinking [a] person’s estimate of the probability of an upcoming outcome, [b] catastrophic thinking [whether the outcome could be managed if it happened][what is the most likely outcome?].
- The patient carries out field experiments to see what actually happens in anxiety-provoking situations, to test the validity of his/her assumptions about the outcome. Experiments can be done in the office, then at home, and in riskier situations.
- If the person is unable to carry out tasks because of skill deficits, he/she needs to learn new skills.
- Teach ways of looking inward, if the person lacks that ability.
- Replace irrational thoughts by rational ones.
29c. Adjunctive Treatment
Cognitive therapy is commonly combined with calming and exposure techniques, and medication is used when necessary. See Section 30. If additional work is needed, psychodynamic therapy can be used next. See Section 28.