SECTIONS: 4 | 6 | 7 | 8 | 9 | 10 | 12 | 13 | 19 | 24

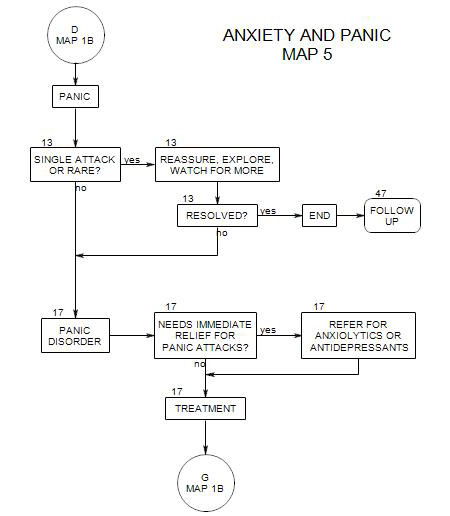
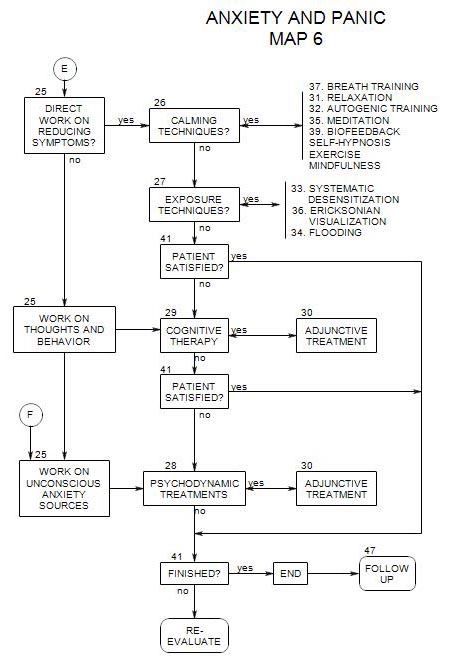
- Comes from the top of Map 6. Coordinates with most treatment sections
A variety of treatment approaches are possible. Here they are divided into-
- anxiety reduction treatments, including calming techniques and exposure techniques.
- cognitive therapy.
- psychodynamic treatments, including psychoanalytic therapy, interpersonal therapy, Gestalt therapy, ego psychology and psychoanalysis.
25a. Paths to relief from anxiety
There are three broad paths to relief from anxiety, as shown on Map 6.
- First try symptom relief. If it is unsuccessful, or if other issues arise in the course of treatment, then try cognitive therapy, and finally, psychodynamic therapy
- Begin with cognitive-behavioral treatment. Bring in symptom reduction treatment as adjunctive. Add psychodynamic work when and if it is needed.
- Start with psychodynamic therapy. When other techniques can be helpful, consider introducing them. Wachtel (1977) discusses this path extensively.
25b. Anxiety Reduction Treatments
These treatments have the common purpose of reducing anxiety levels directly, with little or no attempt to seek out any historical sources or unconscious processes that could be driving them. Use these approaches when you believe that a reduction in anxiety might be a sufficient treatment, because it will free the person to change other aspects of his/her life (Wachtel, 1957, pp. 157, 206).
Such treatments tend to be short-term and focused.
They also can be specified relatively clearly and administered in consistent ways, making it relatively easy to test their effectiveness.
Included here are:
- Calming techniques
- Exposure techniques
Calming Techniques [ Section 26 ]
Here, the specific symptom pattern is not addressed. Rather, focus is on the person’s overall level of tension.
Because specific symptoms often arise in the context of life stress and the person’s difficulty dealing with stress in general, calming techniques are generally helpful and sometimes sufficient. They may be used as the primary treatment modality whenever reducing tension is a goal of treatment, as in generalized anxiety disorder or stress disorder. They may also be useful as adjuncts to other, more focused treatments.
Calming techniques may also be the treatment of choice for temporary relief when no more focused treatment is necessary because the person will recover if the stress is reduced. These are classified as adjustment disorders by the DSM. Long-term relief is provided by environmental change, interpersonal change, treatment of a physical disorder, etc.
However, calming techniques should not be used as the sole treatment for serious disorders, because unmanaged relaxation can provide an opportunity to re-experience the traumatic events that either precipitated or contribute to the patient’s disorder (Linden and Lenz, 1997).
Exposure Treatments [ Section 27 ]
Here, the anxiety-inducing experience is faced head-on, with treatments designed to show the person experientially that there is nothing to fear. The therapist takes an active role in directing the course of treatment, and the patient essentially has only to participate in order to improve.
In general, use exposure treatments when-
- the anxiety is a relatively encapsulated part of an otherwise well-functioning person.
- the patient’s symptoms are externally determined, as in the case of some simple phobias.
- exposure alone appears to be more efficient than alternative treatments.
25c. Cognitive Therapy [ Section 29 ]
Here, it is the person’s own conscious thought processes that are addressed, by focusing on specific things he/she worries about. The premise is that the person’s difficulties are related to errors of thinking. If he/she can be taught to be more rational, he/she can evaluate risks more effectively, and much of his/her anxiety will disappear.
Treatment is based on the premise that what the person is doing or thinking in the present is the primary matter of concern. Once the thoughts and behaviors that sustain the anxiety are modified, the person will be less anxious.
Issues to be addressed include-
- oversensitivity to threat and danger; catastrophic thinking.
- dichotomous thinking.
- personalizing.
- mind reading.
- overgeneralizing.
25d. Psychodynamic Therapy [ Section 28 ]
Sometimes a person’s fears and related behavior appear to be illogical or pointless, or far out of proportion to the precipitating events. We may suspect that the person’s fear is at least partly being generated by unconscious, hidden sources.
In such cases, work on the anxiety symptoms directly or on the conscious meanings of the feared stimuli may be ineffective, because a major component is internally generated and out of awareness. Something more is needed.
Psychodynamic treatment looks underneath the events that precipitated the person’s difficulties for the unconscious meanings of events. Phobic behavior is seen as a consequence of internal conflicts, and treatment explores the origins and meanings of those conflicts. As the internal conflicts are better appreciated and understood, their power to control the person’s actions diminishes, and he/she is more easily able to face situations that had previously been frightening.
In these cases, psychodynamic treatment may be more effective than treatments that work directly on the conscious thoughts and behaviors that are associated with anxiety (Wachtel, 1977, p.192)
Psychodynamic therapy is more likely to be the treatment of choice when-
- symptoms are pervasive.
- the person needs to change lifelong patterns in order to get better.
- symptom reduction treatment has not been effective enough.
- the sources of anxiety are the person’s own thoughts (Wachtel, 1977, pp. 192, 206).
- you need to change the defenses and interaction patterns in order for the symptoms to be reduced.
- the sources of the person’s anxiety or symptoms are long-standing or hidden, and must be uncovered in order to allow the person to work directly on the underlying conflicts or issues.
- your focus is on affective or motivational states (Wachtel, 1977, p.205)
- it is important for the patient to have control over the course of therapy.
25e. Making the Choice
For many reasons, the treatment we provide tends to be a personal choice that each therapist makes for him/herself. However, you may decide to modify the way you operate for some kinds of patients or may even shift your focus over time.
If the optimum treatment strategy for a given patient isn’t something you offer or want to start offering, you can either use an alternative treatment or refer the person to another therapist.
The following is a first attempt to map the choices, according to patient characteristics and treatment limitations:
Anxiety vs. Fear
If the patient is phobic, consider starting with exposure treatment or cognitive therapy. If the person is anxious, consider starting with calming techniques or psychodynamic therapy.
Cognitive vs. Emotional Issues
If the person’s issues are more cognitive, start with exposure treatment or cognitive therapy. If they are ineffective, move on to psychodynamic therapy. If the person’s issues are more emotional, begin with psychodynamic therapy or calming techniques.
Broad Range of Issues vs. Specific Fear or Fears
If the person’s fears are specific, begin with exposure techniques. If more general, start with calming, cognitive or psychodynamic therapy.
Generally Functioning Well vs. Serious Disturbances
Any of these techniques can be used with a person who is basically intact with some fear or anxiety. For patients with serious underlying disorders, it is probably safer to begin with psychodynamic exploration and introduce other techniques as adjunctive.
Time or Financial Limitations
When there are limits imposed on time or patient’s ability to pay, treatment may need to be more symptom-oriented (Almond, 1997, p.168). Having a time limit directs treatment choice toward calming techniques, exposure techniques, cognitive therapy, or short-term, focused psychodynamic therapy.