
-
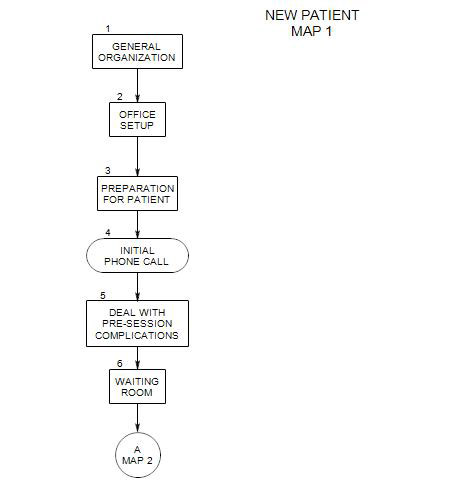
Follows Section 6 on Map 1
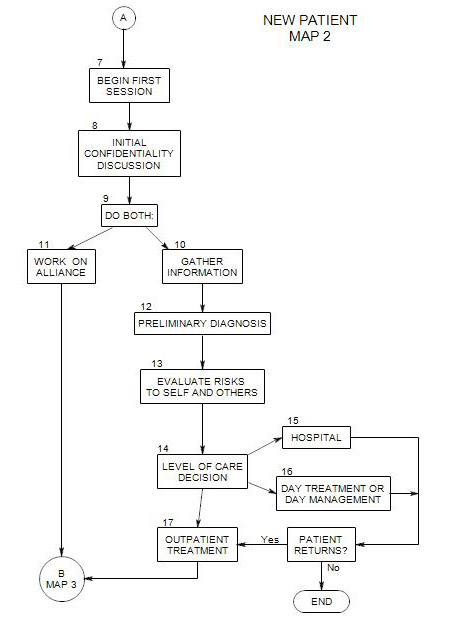
Appears on Map 2
It is difficult to plan a first session, as you typically don’t know the person’s issues, you don’t have a diagnosis, and you may not even know who the patient will be.
Being too loose could lead you to miss important information that you might need in order to establish treatment or fail to tell the person something he/she needs to know. If you are too rigid in your format [like the therapist who told everyone to -lie on the couch and start at the beginning], you could drive some potential patients away. You need to be prepared with basics you want to cover, and open enough to give the person freedom to express what he/she needs to in a way that helps him/her feel comfortable.
You can start with some ice-breakers, continue with the patient’s reasons for being there, and save some time for a discussion of formal and required issues, like payment, schedule, and confidentiality. Start-ups can include
- Introductions
- Some low-key chit-chat can help the person relax and see you as an ally. You can ask about your directions and any problems finding the office; the convenience of the time, who suggested coming to you and why, etc.
- Soon you can ask why the person has come. Most people don’t want either to talk about it or put off talking about it too long, so it’s usually good to get started quickly.
There are a couple of forms in appendices to this section that can be helpful. Appendix A can be copied and taken to the first session, to gather basic data to contact the patient and make insurance claims. Appendix B contains a brief outline of some information about the patient that it can be helpful to collect and compile.
You could print a copy of Appendix B for each patient and fill in whatever information you need between sessions. Then you can review the compilation from time to time. As a way of organizing your thinking about the patient. Having the categories on a form helps you notice what you have learned the most about the patient and what has not been discussed.
Organization of Session [see Lucas]
- Indicate the length of the session, and possibly something about what you need to know, how you operate, or how the session can progress
- If you expect the first session or two to extend beyond your usual time frame, it might help to mention that at some point.
- If you take notes, this might be a good time to comment on it, and lead to a brief statement about confidentiality
- Some comments about confidentiality and its limits should be made before the discussion of substantive issues begins, if for no other reason than to reassure the patient that you consider these issues important and will respect his/her privacy. Confidentiality is of course limited by safety, legal considerations and the person’s prior commitments to his/her insurance and managed care companies.
- Often you can gather the basic information you need in the course of the session. If not, stop the person with enough time to fill in the data you need.
- Also leave time for summing up, planning for subsequent sessions, dealing with payment and/or insurance, answering any questions the patient may have, etc. Here is where Appendix A to this section can be helpful.
- You can ask if the patient has any questions about you, your training and experience, etc. If he or she goes too far, it can be an interesting starting point for treatment [How would that be helpful to you?]
- Expect your patient to notice whether you have ended when you said you would and to expect the same from you in subsequent sessions.
Goals of First Session[s]
A number of things need to occur simultaneously in the first session[s]. You must:
- work on your alliance with the patient[s]. This will be discussed in Section 11: Alliance Building.
- deal with initial resistances. This is also discussed in Sect. 8
- gather information that allows you to make crucial decisions about the treatment. See Section 10: Gather Initial Information, Section 12: Preliminary Diagnosis, Section 13: Evaluate Dangers, and Section 14: Level of Care for discussions of these issues.
- provide information that helps the patient[s] make his/her/their choices about treatment. This could include discussion of fees, time availability, travel to your office, alternatives to psychotherapy, your style and approach. The person will of course notice your style and approach during the session and will be making up his/her mind about them as the session progresses.
- begin to offer help – or at least, the possibility of help – with the patient[s]’ issues.
- start to explore issues related to the patient’s choice to pursue treatment at this time. In addition to practical matters and resistances, it might include a discussion of various approaches to the issues presented and whether you are the person to work with him/her on them.
The Participants
The session will unfold differently, depending on who is present. It is important to keep in mind who the patient is; it could be an individual, a couple, or a family. If a patient comes in with his/her spouse, the situation is quite different from dealing with a couple as the patient.
Patient Alone
This is the situation covered by the current map.
Patient and Another
- You need to develop an alliance with both the identified patient and the other(s) in the session.
- Establish who the patient is [could be the couple, the family]
- Note that, if the other isn’t a patient, confidentiality may not apply. You may want to raise this issue with both patient and other.
Patient is a Couple or Family
Split Session
7 Appendix A:
It can be helpful to have a printed copy of this form when you meet with a patient for the first time. It calls for some basic information that allows you to get in touch with the person and make claims to the insurance company. Much of this can be skipped if the patient is self-paying.
PATIENT INSURANCE INFORMATION
Patient Insured
[if different]
Name _____________________ ___________________
Address _____________________ ___________________
Town _____________________ ___________________
State _____________________ ___________________
Telephone _____________________ ___________________
Telephone _____________________ ___________________
Birth Date _____________________ ___________________
Sex _____________________ ___________________
Employer _____________________ ___________________
Initial Call _______________ Date of First Session______________
Patient’s Relationship to Insured__________________
Insurance Company and Plan___________________________________
Insurance ID _____________________________
SS # _____________________
Referred by______________________________
Managed?________
Precertify?_______Preauthorization Number ____________________________
Deductible?_____________________ Copay______________________
Diagnosis:____________________________________________
Secondary Insurance?______ if so, then-
Plan___________________________________________________
Pt ins info
7 Appendix B: Data Record for New Patient
The recommendation here is to collect information as you go and fill in the form between sessions. Fill in whatever looks like it could be helpful, and leave the rest blank.
The form can provide a reminder of some of what you have learned already about the patient, help you put the information together into a pattern, and suggest other information you may want to ask about.
This listing is in addition to the information on the form in Appendix A
Name
Notes through
Stuff to Cover Early On
Insurance
Fee, how paid
Length of session
Frequency of sessions
Confidentiality
Note taking
Professional info about the therapist
Reasons for coming
Symptom History
Wants and Goals
Strengths and Resources
Prior Therapy or Hospitalization
Coordination with other professionals or agencies
DSM
I:
II:
III:
IV:
V:
Defenses
Medical
Drugs, Alcohol, Tobacco
Living Conditions
Daily Routine
Financial
Education
Legal
Work
Work History
Avocations
Current Family or Relationships
Relationship History
Family of Origin
Parents
Mother
Father
History
Recent History
Friends
Religion