SECTIONS: 5 | 8 | 16 | 19 | 21 | 22 | 24 | 25 | 39 | 44 | 46 | 47 | 48
SECTIONS: 8 | 28 | 29 | 30 | 32 | 33 | 34 | 35 | 36 | 37 | 39

-
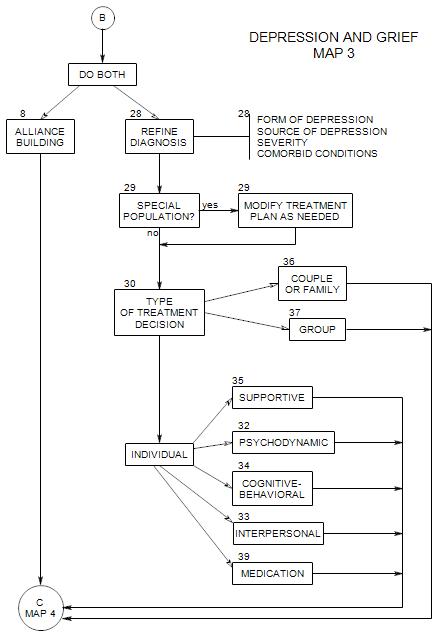
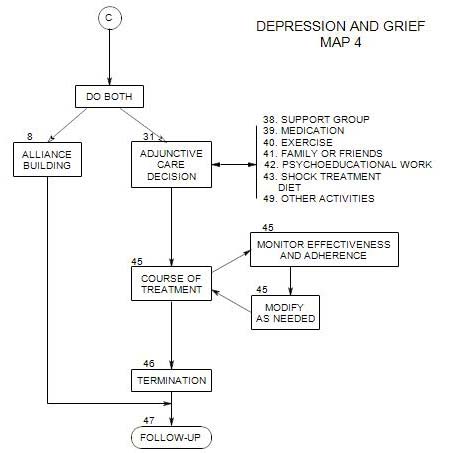
This decision follows after and from your decision regarding the primary form of treatment, Section 30 on Map 3. It appears on the top of Map 4.
Once the form of primary treatment has been decided upon, you need to consider what, if any, additional care can be helpful to the patient.
It may include making life changes, such as
- joining a support group [ Section 38 ]
- developing new connections with family or friends [ Section 41 ]
- an exercise program [ Section 40 ]
- change of diet
- meaningful activity
It may also include biological treatments such as
- antidepressant or other medication [ Section 39 ]
- electroconvulsive shock [ Section 43 ]
31a. Support Groups
Depressed people commonly feel very alone and lonely. They may also avoid others, thus creating or increasing their sense of being different, unworthy, strange, rejected, etc.
A group of others who have similar issues can lessen the sense of uniqueness and alienation. Group members can support one another in many ways, through understanding, outside contact and help, social events, etc.
31b. New Connections with Family and Friends
31c. Exercise
31d. Change of Diet
31e. Meaningful Activity
31f. Medication
We have some ambivalence about whether medication is adjunctive care or an integral part of primary treatment, because the answer depends on whether there appears to be a biological component to the patient’s depression, along with the patient’s level of depression and ability to cope with it.
Potential advantages of medicating
- reduce symptomatology
- help the patient feel better
- help the patient cope more effectively with everyday life
Potential advantages of not medicating
- ―use the patient’s distress as a motivator explore
- ―interpersonal and intrapsychic sources of the distress
Risks of medicating could include
- giving a nonverbal message that the patient’s issues are primarily biological or that the patient is too disturbed to be helped psychotherapeutically.
- supporting the idea that therapeutic work isn’t necessary
Risk of not medicating might include
- ―patient’s inference that s/he is not being taken seriously
- ―patient’s actually being so depressed that s/he can’t manage his/her life effectively, and gets worse.
SIGNS OF A BIOLOGICAL COMPONENT THAT ANTIDEPRESSANTS COULD HELP
- Fatigue
- Sleep disturbance, especially:
―several awakenings each night
―early morning awakenings, difficulty returning to sleep
―excessive sleeping or lack of sleep
- Decreased sex drive
- Consistent mood changes throughout the day – usually feeling better as the day progresses
- Extreme inability to feel pleasure
- Forgetfulness
- Difficulty concentrating
OTHER USES OF MEDICATION
- Anxiolytics to manage anxiety that has precipitated the depressive episode
- Hypnotics when sleep loss is a significant factor in the patient’s mood, ability to concentrate, etc.
- Medical treatment of other biological disorders that are contributing to the patient’s mood
Additional Issues That Should be Addressed
- Whether to refer to a psychiatrist or internist
- What to tell the psychiatrist or internist
- What to tell the patient about medication
- How to deal with any medication issues that arise.
These are discussed in Section 39.
31g. Shock Treatment
Electroshock treatment is more expensive and less available than medication. However, in some cases it may be safer, in its current form, than medication. It may in fact be the treatment of choice for the elderly, pregnant women, and patients with dementia or serious illness.
The primary risk, memory loss, is usually temporary and not disabling.
There is a relatively high probability of relapse following shock treatment; however, it can be reduced by maintenance treatment or psychotherapy.