
-
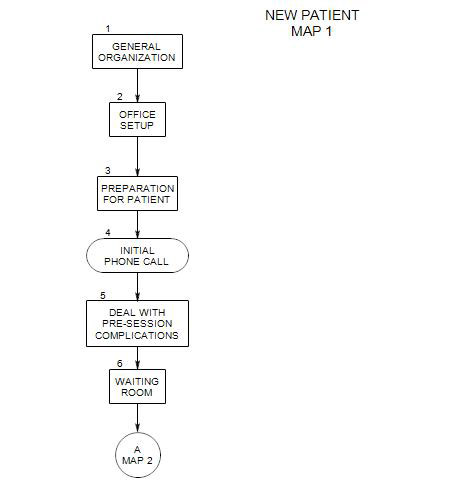
Follows Section 3 on Map 1
4a. The Basics
The primary purpose of the initial phone call is to determine whether you are the right person for the prospective patient; then either make an appointment or send the person on to a more appropriate therapist or facility.
In some sense, both diagnosis and treatment begin as soon as you answer the telephone. You are gathering information about the patient that will inform your next encounter with the patient. You are also providing information about therapy and how you work. You also have to assume that the caller is paying attention and will make some use out of whatever you say.
There are some things you can do in the briefest of calls, others that are optional. You probably have the option of returning or continuing the call at a later time; or you may address some of the issues during the initial appointment. You may want to have a form ready, near your telephone, to make sure that you cover all necessary issues.
Important pieces of information include:
- The caller’s name and relationship to the prospective patient – if they are different
- The prospective patient’s name
- The reason for the call
- The degree of urgency in getting started
- How the caller got your name
- The caller’s telephone number
In addition, you should-
- determine the prospective patient’s ability to pay for treatment
- make a first appointment
- give directions to your office
Get a first idea of the reason for the call. What does the caller want from you? The amount of information you take at this time depends on several factors:
- Your time pressure and availability.
- The caller’s urgency.
- Your wish to gather information later, in an appropriate setting, and not train the person to expect telephone consultations.
You can get a quick sense of your appropriateness for this patient:
- Is the patient coming with issues that you probably can treat, or does he/she need other services?
- Does the person want services that you can provide? If not, can you be helpful anyway, and should you try to steer the patient toward related work that you can help with?
- Can the patient pay your fee? Some prospective patients will ask if you take their insurance. You can state your fee at this time; then if the person says OK, you have a basis for moving forward. If not, you will have to decide whether to negotiate at this time or defer to the first session.
You could ask how he/she got your name, which could lead to the name of the referral source and more information about the person’s expectations of you. If the person got your name from a list, like the phone book, it might pay to ask how he/she picked out your name. Perhaps the caller has heard of you or knows someone who came to you in the past. Perhaps it was something about your listing, the sound of your name, etc. This may also be related to the caller’s expectations of you.
Make a first appointment – the sooner the better, within the limits of your schedule and the patient’s schedule and ability to get to your office. You should have your appointment calendar ready.
Get telephone numbers (in case you need to reach the patient for any reason, e.g.: to change the appointment)
Give directions to your office. This can be a mini-opportunity to start getting comfortable talking with one another. If the directions are complicated, you can also get the caller’s address or fax number and send him/her a map or suggest that he/she consult an Internet map service such as MapQuest.
4b. The Process of the Call
Your next job is to make it easy for the patient to come to the first appointment. This involves-
- appreciating that the caller may have had some difficulty making the call.
- helping the caller feel comfortable with you and the idea of therapy.
- reassuring the caller that you can provide some help.
- working through the details of making the appointment.
Your own telephone answering style will affect the way you handle these issues. In general, it probably is helpful to be-
- ―informal, so he/she won’t have to overcome the barrier of formality to talk with you.
- ―available for an immediate consultation at [as much as possible] his/her convenience.
- ―respectful, so the person knows that his/her issues will be taken seriously.
- ―encouraging, that you are capable and prepared to provide the help he/she needs.
4c. Additional Information
Be prepared to deal with the caller about your fee. Many patients who are paying for their own treatment believe that they must shop around for the best price. You may want to encourage patient to make an informed choice of therapist, including consideration of therapist’s background and special training, and how comfortable they feel with the therapist. These considerations apply even when the choice of therapists has been limited by some arbitrary third party. Invite the person in for an intake session.
You may also want to tell the person your fee for the first session, especially if your fee is higher than other therapists, or if your practice is full and you don’t want to take any new patients at reduced fee.
Ask about insurance. If you are not part of the patient’s insurance panel, seeing him/her can involve extra costs to the patient. If the patient has managed care, you should check on the formal and likely limits to coverage (these may be very different!), as a basis for designing your treatment. Some insurance plans require that the patient call in ahead of the first session, and it would be helpful if you knew those requirements.
You should also consider covering:
- Whether the initial appointment will be for a consultation or the beginning of treatment, or whether you want to leave that open. Commonly, people only wanting a consultation will say that, and it can help you structure the initial session.
- The length of first session. This will help the caller plan his/her time for the day of the appointment.
- Whether the person has records to bring to the first session, especially if this is a hospital or insurance referral.
The caller may have questions also. These must be taken seriously but not necessarily at face value.
- Questions about your fee and insurance should be answered directly
- Questions about your training may have to do with the issue of whether you are good enough. You may have to decide whether to respond with facts or an interpretation.
- Questions about your style and theoretical orientation may have to do with the caller’s expectation or previous experience in treatment.
4d. Some Complications
The person calling has already made several steps to get there: deciding on the need to call, getting your name and telephone number, and actually calling. In the course of doing this he/she has had to deal with a variety of issues, internal and external, that have worked against making the appointment. You don’t know what those issues are, but there are some common ones to watch out for.
External issues can include-
- costs of treatment.
- time commitments and pressures.
- pressures from others [esp family] to come or not to come.
- job pressures [e.g.: police officers may face job constrictions, such as the ability to carry a weapon, if they admit to being in psychotherapy].
- legal mandates to go for treatment.
In addition, there are always internal resistances to beginning treatment [see Strean, ch.3]. Specific reasons for avoiding therapy can include
- the idea that a therapist can take control over one’s life.
- reluctance to change oneself or fear of having to change.
- embarrassment at having to reveal sexual and other secrets.
- fear that you will reveal something about him/her to others, especially family or employer. You may need to reassure the caller about confidentiality, if this comes up.
- sense of having to admit failure in some important aspect of one’s life.
How much you try to handle during an initial telephone call depends on a number of factors
- the caller’s apparent urgency.
- whether you are in session or otherwise unavailable to talk.
- your general style.
- a sense that you may be able to make a better connection with this caller by staying on longer.
- a feeling that additional conversation will help this person come to see you.
- your sense that the caller is looking for excuses not to come.
Evidence of resistance on the telephone can include-
- asking detailed questions about your fee policy, your time availability, your training, your theoretical perspective, etc.
- insisting on a particular type of treatment
- making other impossible demands about the treatment conditions [e.g.: asking for an appointment time when most therapists can be expected to be unavailable; wanting you to have sessions in the patient’s home; etc.]
There are a number of things you can do to deal with resistances during the initial phone call:
- Take each demand or request seriously but not necessarily at face value.
- Try to make therapy seem safe.
- Normalize the patient’s resistance [You know, it’s not unusual to have second thoughts about starting therapy.]
- RE: questions: you can always say that the issues are important and that you would prefer to discuss them in person.
- RE impossible demands: suggest that treatment may be inconvenient and difficult for the person right now, and ask if he/she wants to postpone coming to a better time.
- Suggest that the person come in for a consultation, so you can decide together the most effective path to pursue.
4e. Some More Complications
If the caller is not the prospective patient, it raises some additional issues. You may want to ask them, and see what develops. [Is it important for me to know why your husband didn’t make the call himself?]
- It might reflect the prospective patient’s inability to make a call, due to a variety of reasons, physical or psychological.
- Perhaps the caller is pressuring the other one to come for treatment, and you will be an instrument in some kind of power play in the relationship.
- Perhaps the prospective patient treats the caller like a servant, the caller is resentful, and a suggestion of couple treatment will be received with relief.
- Perhaps this person is unconsciously looking for help but must act it out in an indirect way. If you suspect that this is the case, Strean suggests inviting the caller in for further consultation, with the possibility of making him/her the patient.
A number of issues may have prompted the call that also might lead you to suggest inviting a significant other to the first session. If you ask about the reasons for the call, you will have an opportunity to decide:
- drug or alcohol misuse
- relationship problems
- complaints about the other person
- For another discussion of the initial phone call, see Silverman, 2005.